
A decade of international research has led to a significant shift in the medical understanding of polycystic ovary syndrome (PCOS). The condition is now no longer viewed solely as a gynecological disorder, but as a multi-system metabolic phenomenon that can help explain symptoms such as obesity, excess hair growth and diabetes. Accordingly, its name has also been changed to PMOS — Polyendocrine Metabolic Ovarian Syndrome.
The move follows years of discussion, research and international collaboration led by experts in women’s health and endocrinology. It was first presented at the European Congress of Endocrinology held in Prague last month and later published in the medical journal The Lancet. The decision was based on surveys, focus groups and consultations involving more than 22,000 participants — including physicians, researchers and women living with the condition — who argued for years that the existing name was misleading and did not reflect the complexity of the disorder.
Gallery
")
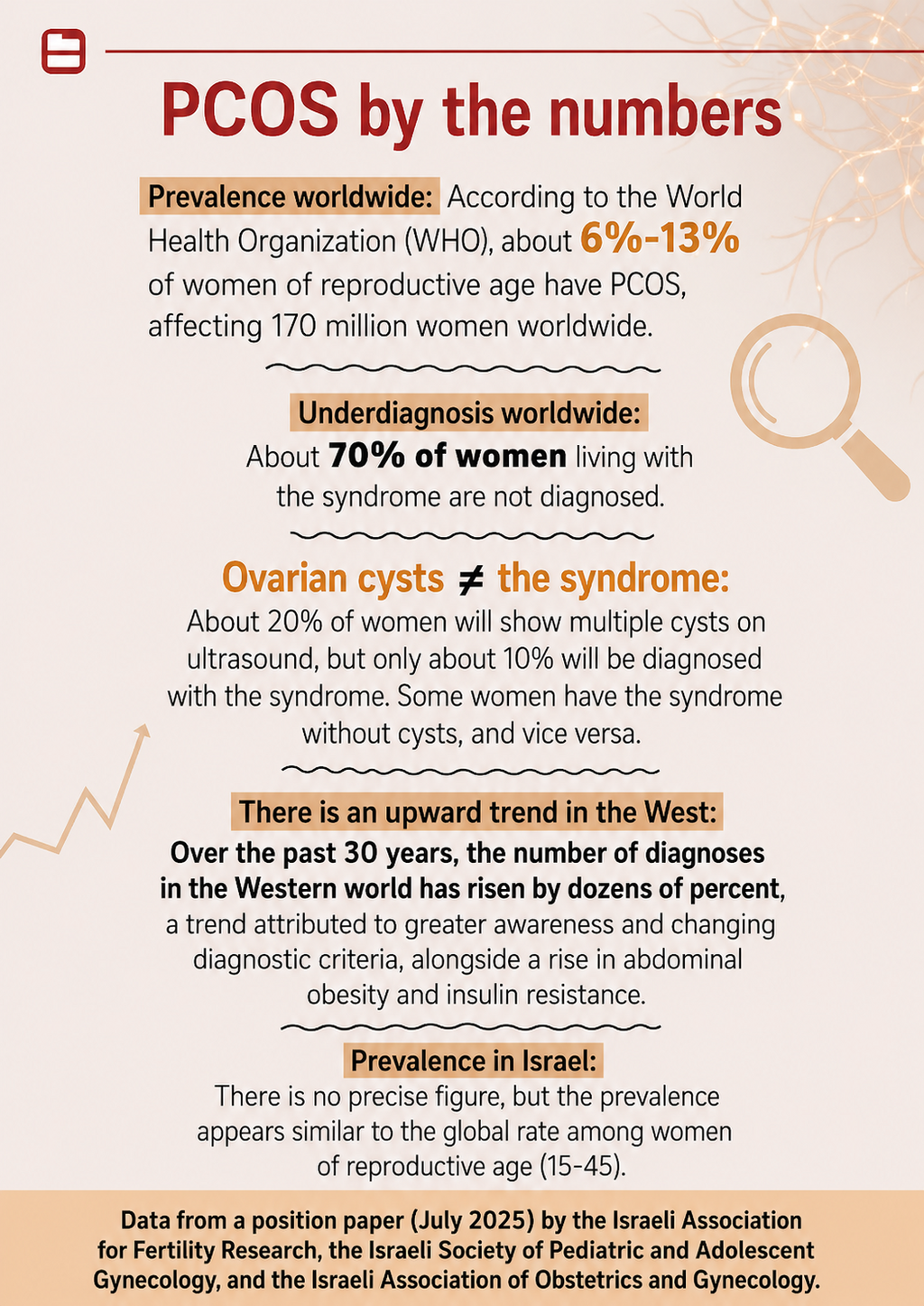
PCOS is no longer viewed solely as a gynecological disorder, but as a multi-system metabolic phenomenon
(Photo: Shutterstock/ASAP Creative )
Lead researcher Professor Helena Teede of Monash University in Australia said the old name had created a misleading understanding of the disease, as if it were solely an ovarian problem.
“For a long time, the name reduced a complex long-term endocrine disorder to a misunderstanding around ‘cysts’ and an excessive focus on the ovaries,” she said. “The new name better reflects the systemic and ongoing nature of the condition.”
Dr. Galina Shenkerman, an endocrinology and internal medicine specialist and medical director at MEDBALANCE, a metabolic diseases center, agreed that the new name better reflects the condition’s complex nature, which affects not only the reproductive system but also metabolism and the risk of diabetes and other metabolic diseases. She said the previous focus on the ovaries had for years led to an incomplete clinical picture.
“Studies have shown that these are not actually ovarian cysts, but follicles that fail to mature and progress to ovulation,” she explained. “The problem stems from a deficiency in female hormones and an increase in male hormones, which cause external symptoms such as excess hair growth, but also insulin resistance, weight gain, acne, fertility difficulties and an increased risk of type 2 diabetes.”
According to her, despite a strong genetic component, lifestyle change plays a central role in treatment.
“When I began my endocrinology residency more than 20 years ago, a patient came to see me with this condition,” she recalled. “She told me she and her husband had been trying to conceive for seven years, including IVF treatments, without success. I told her there were other possible causes, so we should run tests, but in the meantime she should switch to a diet aimed at weight reduction and increase physical activity to lower insulin levels. Even before all the test results came back, she lost 10 kilograms and became pregnant.”
How was the condition diagnosed until now?
“In many women, diagnosis usually begins with what appears to be a menstrual irregularity or difficulty conceiving — two classic reasons for visiting a gynecologist. However, what is later discovered is often a much broader picture: a combination of hormonal and metabolic changes that can also manifest as acne, excess hair growth, hair loss, fatigue or difficulty maintaining a healthy weight.”
Will the diagnostic process change?
“There will not be an immediate change. According to the World Health Organization plan, it will be implemented in daily practice within three years, as this is the timeframe required for changes in disease classification, training of medical and administrative systems, translations into all languages and cultural adaptation.”
What can a woman expect at a gynecologist visit for fertility issues?
“As mentioned, diagnosis that previously focused on the gynecological aspect will now also include the metabolic side. In addition to ultrasound, the patient will undergo tests for female and male hormones, levels of pituitary hormones called gonadotropins, insulin levels, and general tests for disorders of sugar and fat metabolism. When there is already suspicion of a hormonal disorder, the patient should be referred for a glucose tolerance test, which can determine whether pre-diabetes is present and allow tailored treatment.”
Why does the condition lead to weight gain?
In a normal state, the pancreas secretes insulin according to the amount of carbohydrates consumed. In PMOS, the pancreas secretes excessive insulin that is unable to effectively reduce blood sugar levels — a condition known as insulin resistance.
Because blood sugar levels remain high, the pancreas receives a signal to secrete even more insulin, creating a cycle of chronic overproduction. This resistance is now considered a central driver of the condition and of weight gain that is extremely difficult to treat.
High insulin promotes weight gain and blocks weight loss in two ways: by increasing hunger and the craving for sugar and carbohydrates, and by stimulating fat tissue formation while inhibiting its breakdown.
The higher the body’s fat mass, the more severe the insulin resistance becomes and the higher insulin secretion rises, making weight loss even more difficult.
To break this cycle, fat mass must be reduced and insulin sensitivity improved through a carefully tailored diet and physical activity.
What should you eat?
- Consume only whole carbohydrates, such as quinoa, legumes, whole grain bread, whole grain cereals, etc.
- Start and end the day with protein and minimal carbohydrates.
- Limit carbohydrates to 40% of daily caloric intake (as calculated by dietitians) and increase protein at the expense of carbohydrates.
- Do not spread carbohydrate intake throughout the day as in many diets, but concentrate it in one or two meals.
- Create a “protein window” during which only protein is consumed (see recommended plan). This window should last as many hours as possible. During this time, the pancreas is not exposed to sugars, insulin levels drop, and fat breakdown becomes possible.
- Consume dairy products with up to 5% fat only. According to Chinese medicine, preference should be given to sheep and goat dairy products.
- No more than one egg yolk per day, sometimes less, depending on professional guidance.
- Eat fish.
Physical activity: mandatory
Exercise is essential, not only for calorie burning. Physical activity helps reduce insulin levels in women with the condition, leading to fat breakdown and reduced body fat percentage. A combination of aerobic exercise and strength training is recommended and has been shown to be effective in managing the condition.
1,300 calories per day
Sample daily menu for weight loss in PMOS
Breakfast:
Whole grain bread with 5% cheese spread + vegetables, or a cup of unsweetened whole grain cereal + half a cup of milk.
Snack:
Fruit + yogurt.
Lunch:
Lean protein (non-fried, skinless chicken/turkey/fish, 150g), or tuna can, or yogurt + egg / 250g 5% cheese, plus raw and cooked vegetables (excluding potato, sweet potato, peas or corn).
Snack:
Diet dairy dessert or diet ice cream.
Dinner:
Start with a glass of water/soda/herbal caffeine-free tea, followed by vegetables + one carbohydrate option: whole grain bread / rice / whole wheat pasta / barley / couscous / bulgur / legumes.
Or: egg / yogurt / 100g 5% cheese / half a can of tuna or sardines.
Throughout the day:
- Half a cup of milk and 10 cups of sugar-free drinks (tea, decaf coffee, water; minimize diet drinks).
- Two servings of fruit per day (e.g., orange, apple, pear, peach, two clementines, 10 strawberries or cherries, 15 green grapes, two kiwis, half a cup of blueberries, or two plums). Preferably combined with carbohydrate meals.
- Twice daily, choose one fat portion: a tablespoon of oil or mayonnaise / 2 tablespoons of tahini or light mayonnaise / 10 olives or almonds / 5 walnuts or pecans / quarter avocado.
- Once daily snack: 3 cups popcorn / ice cream cup / granola bar / 2 slices whole grain bread with fruit-only jam, preferably with carbohydrate meals.
- Avoid fried foods, nuts, fatty snacks, cakes, full-fat cheeses, puff pastry, sugary drinks, white flour products, white sugar, caffeine, chocolate and alcohol.
- Stop eating two hours before sleep.
The plan is based on the principles described in the article. It is intended for healthy women aged 18 and above, not for pregnant or breastfeeding women, and does not constitute medical or nutritional advice.