
When a two-day-old baby begins having seizures, the last thing most parents, and sometimes even medical teams, think of is stroke. But that is exactly what can happen, and more often than many people realize. One in every 4,000 newborns suffers a stroke around birth, a rate higher than that of well-known genetic diseases routinely screened for in newborns.
“People are surprised to discover how much less rare stroke in children is than they think,” says Dr. Moran Hausman Kedem, head of Pediatric Neurology Institute, Pediatric Stroke and Cerebrovascular Disease Unit at Tel Aviv Sourasky Medical Center's Dana-Dwek Children's Hospital. “We are talking about six to 12 cases per 100,000 children each year, and about 50% of all childhood strokes occur in the first year of life.”
")
What is a stroke?
A stroke is an acute neurological event in which blood flow to an area of the brain is suddenly interrupted, causing damage to brain tissue. There are two main types: ischemic stroke, in which a blood vessel is blocked by a clot that forms locally or travels from another part of the body, and hemorrhagic stroke, in which a blood vessel ruptures and causes bleeding in the brain. In children, unlike adults, hemorrhagic stroke accounts for a relatively high share of cases.
Most parents whose baby suffers a stroke will not know it in the delivery room. The birth itself usually unfolds without drama, the baby appears healthy, and the signs typically appear only toward the end of the first day of life, usually during the second day.
“Usually it will be a focal seizure, jerking of one arm or one leg, or pauses in breathing, which are one of the ways seizures can appear in babies,” explains Dr. Hausman Kedem. “A focal seizure always raises suspicion that there is a focal process in the brain.”
The most common cause at this age is an embolus from the placenta, a clot that forms in the placenta and travels through the bloodstream to the brain. It does not mean something went wrong during pregnancy, and it does not mean the birth was difficult.
") Dr. Moran Hausman KedemPhoto: Private
Dr. Moran Hausman KedemPhoto: Private“We tell parents that it is not their fault and that there was nothing else they could have done,” she says. “In most cases, the event cannot be prevented, and we see it even in completely healthy young women with a placenta that appears normal.”
Smoking and diseases that affect the placenta, such as preeclampsia, inflammation or infection, can increase the risk, but in most cases the cause is not something that could have been prevented.
In addition to the placenta, congenital heart defects, especially cyanotic cardiac defects in which non-oxygenated blood passes from the right side of the heart to the left, sometimes carrying a clot that can reach the brain and block a blood vessel, are also linked to a higher risk of cerebral infarction. Infections, inherited clotting disorders and birth trauma are less common causes.
The good news is that when the source is the placenta, the risk of recurrence is very low. “If there is no heart defect and no congenital disorder of the blood vessels, the chance that it will happen again is practically zero,” Dr. Hausman Kedem explains. “And it is very important to explain that to parents.”
Treatment differs from adults
In the first stage, doctors treat and stabilize the baby with supportive care and anti-seizure medication, while also trying to identify the cause, because that will determine the risk of recurrence. The tests include an echocardiogram and a brain MRI with imaging of the blood vessels, and in rare cases, testing to rule out hypercoagulability.
Unlike in adults, babies are usually not given clot-busting drugs or blood thinners unless a specific cause is found, such as a heart defect or a congenital disorder of the blood vessels. The reason is that often, by the time the infarction is detected, the clot has already dissolved and the blood vessel has reopened on its own.
Stroke in a baby sounds like an unavoidable disaster, but the picture is more complex. The young brain has a healing ability the adult brain does not: neuroplasticity, the ability to reorganize and allow healthy areas to take on functions that were damaged. “Entire areas can take over functions that were lost,” says Dr. Hausman Kedem. “That is something an adult brain cannot do.”
But “better” does not necessarily mean “normal.” In about 60% to 70% of cases, some neurological injury will remain, most often one-sided motor impairment, known as unilateral cerebral palsy: asymmetry in walking, spasticity and weakness. In other cases, children may develop sensory, language, vision, hearing or attention disorders, learning disabilities, behavioral disorders or epilepsy.
In preschool and school-age children, stroke may initially look like something else entirely. A child arriving at the emergency room with sudden weakness in one arm may first be suspected of having an elbow dislocation. Only when additional neurological symptoms appear does the real picture become clear.
")
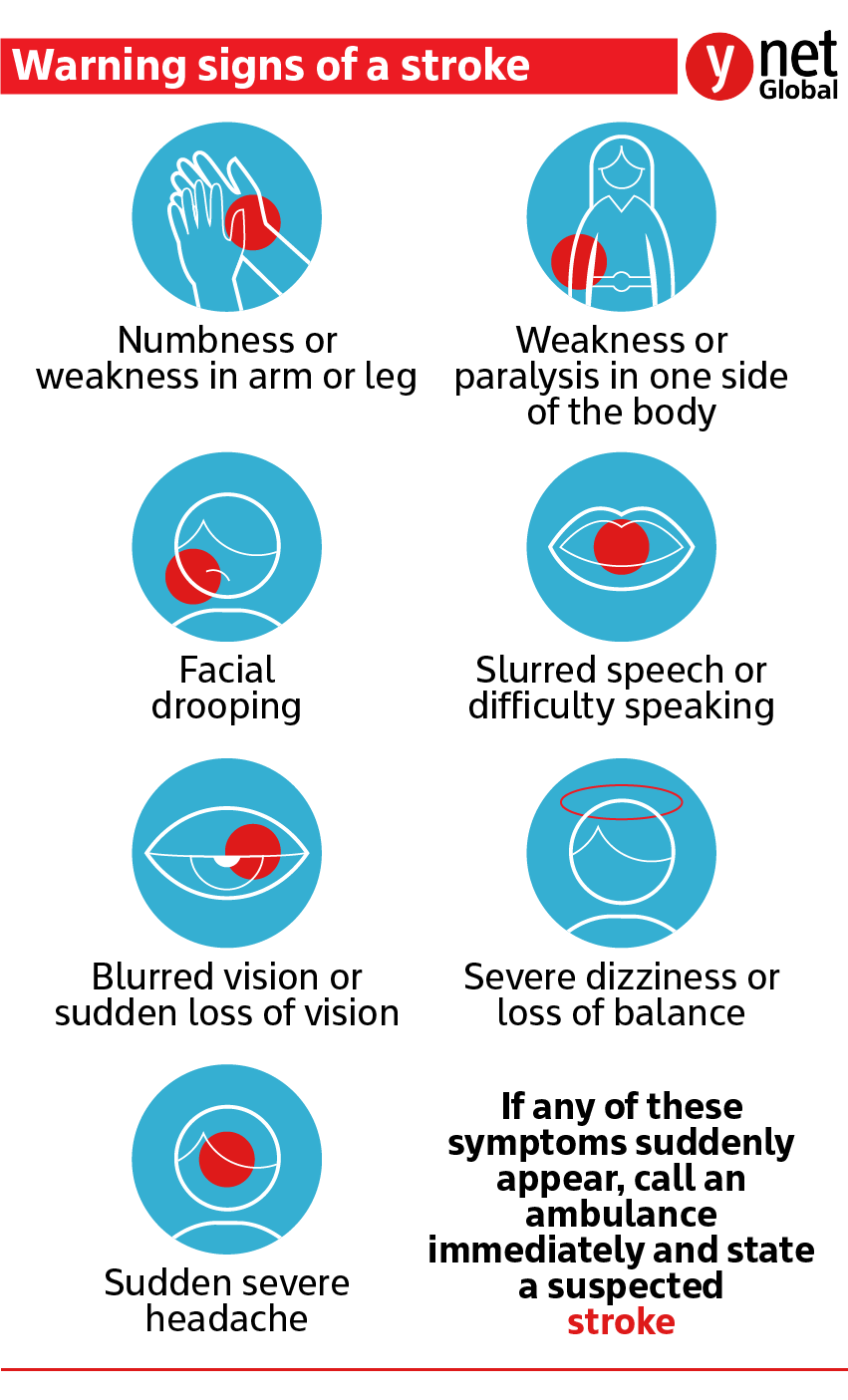
Which symptoms require urgent evaluation?
(Photo: Sabphoto / Shutterstock)
“When the face is involved, such as drooping at the corner of the mouth or one-sided facial weakness, the diagnosis usually comes faster,” says Dr. Hausman Kedem. “But the principle is the same as in adults: time is brain. Every minute that passes translates into the loss of about 190 million nerve cells.”
The causes at this age are entirely different from those in babies: vasculitis (inflammation of the blood vessels); brain infections; clotting disorders; head trauma; and rare diseases such as moyamoya, which is sometimes treated with surgery to create alternative blood vessels. Hemorrhagic stroke in children is usually caused by a congenital vascular malformation that had remained silent for years and ruptured without warning, such as an AVM (an abnormal connection between an artery and a vein); an aneurysm; or a cavernoma.
In January 2026, the American Stroke Association published updated guidelines that, for the first time, include recommendations specifically for children: adapted diagnostic protocols, official recognition of the need for dedicated treatment systems and approval for mechanical clot removal from brain blood vessels in selected cases, a treatment that until now has mainly been used in adults.
Dr. Hausman Kedem stresses that temporary neurological symptoms in children are not necessarily a stroke, so there is no need for panic. But one sign requires urgent medical attention without hesitation: suddenness.
Sudden one-sided weakness in the face, arm or leg, sudden difficulty speaking, sharp facial asymmetry or sudden difficulty walking in a child who had been completely well moments earlier all require urgent evaluation.
“A neurological symptom that appears suddenly, without gradual development, in a child who was perfectly fine a moment earlier, is the red flag,” she says. “And in babies, any focal seizure, repeated jerking of one arm or one leg, requires urgent evaluation.”