
For many years, epilepsy treatment rested on one simple principle: trial and error. After diagnosis, doctors chose an anti-seizure medication according to the type of seizures. If control was not achieved, another medication was tried.
For many patients, that approach worked. But for others, especially children with severe epilepsy, it meant years of uncertainty, recurrent seizures and damage to development and quality of life.
Gallery
")
Epilepsy treatment enters a new era as doctors look for the disease’s genetic cause
(Photo: Shutterstock)
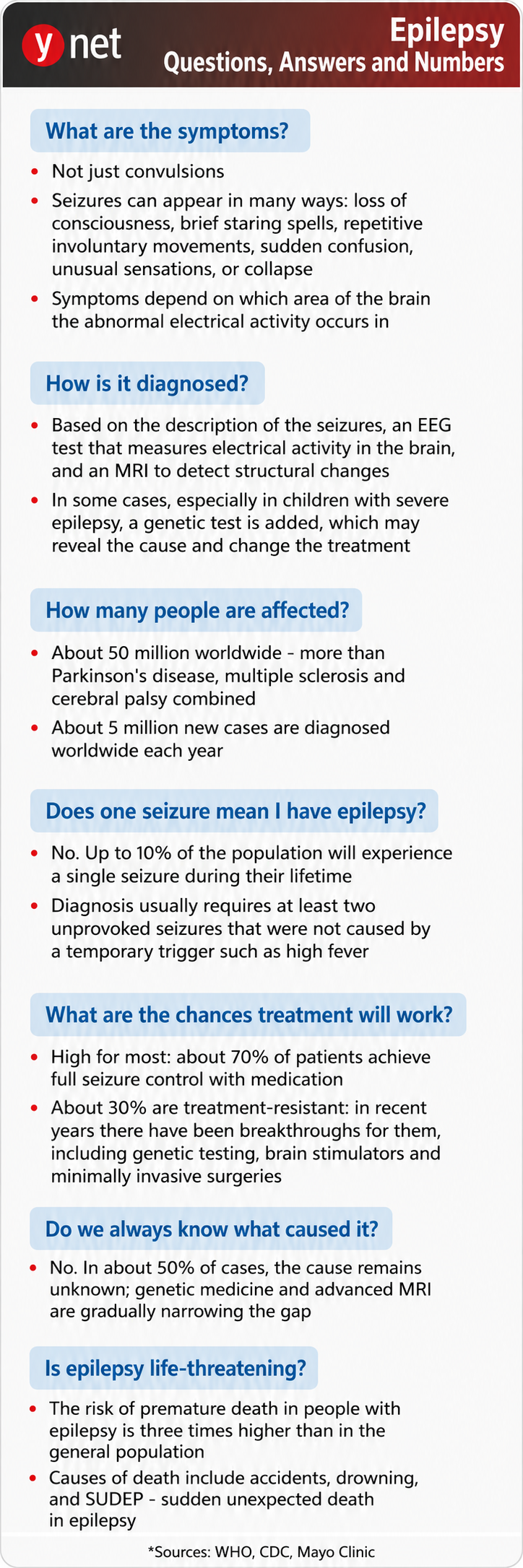
Epilepsy is one of the most common neurological disorders, affecting about 1% of the population. Although most patients achieve good seizure control, about one-third continue to suffer despite optimal drug treatment. In recent years, it has become clear that in a significant share of cases, especially among children whose disease begins at a young age, the cause lies in genetic changes that affect the activity of nerve cells in the brain.
Advances in genome sequencing technologies have fundamentally changed the picture. What once ended with the frustrating answer, “We do not know why this happened,” can now become a precise diagnosis, and sometimes a key to treatment.
Today, instead of asking only, “Which drug can reduce the seizures?” doctors are asking a different question: Why did this patient develop epilepsy, and can we treat the cause itself? That is the heart of personalized medicine.
Treating the cause, not only the result
Genetic testing is not intended for everyone, but its use is expanding. Today, doctors commonly consider genetic evaluation in children whose epilepsy began at a young age, in cases resistant to treatment, when there is developmental delay or intellectual disability, when there are findings outside the nervous system, and when there is a relevant family history.
The test is not meant only to provide the family with an answer. Often, it can change treatment in a very real way.
Dravet syndrome is one of the best-known examples. It is caused by a mutation in the SCN1A gene and usually appears during the first year of life. Early identification of the diagnosis allows doctors to avoid drugs that block sodium channels, which can worsen the condition, and choose more appropriate treatments.
GLUT1 deficiency syndrome is very different. It is caused by damage to the gene responsible for transporting glucose to the brain. Here, the problem is the fuel reaching the brain. Genetic diagnosis leads to an entirely different treatment: a ketogenic diet, which provides the brain with an alternative energy source. For some children, this treatment can enable good seizure control and even significant functional improvement.
One of the most impressive examples of personalized medicine is tuberous sclerosis complex, or TSC. This genetic disease can manifest in epilepsy, developmental delay, autism spectrum disorders and benign tumors in the brain, kidneys, heart, skin and lungs. For years, treatment focused mainly on controlling seizures and monitoring the complications of the disease.
Understanding the molecular mechanism changed the picture. Researchers found that the genetic defect causes increased activation of an intracellular pathway called mTOR, which regulates cell growth and division. Following that discovery, drugs were developed to inhibit this pathway, led by everolimus.
These drugs do not treat only the seizures. They target the disease mechanism itself, and can reduce seizure frequency and even shrink brain and kidney tumors. TSC became one of the first proofs that understanding the genetics of a disease can lead to focused, precise treatment.
Editing the genetic code
One of the most fascinating areas today is the development of treatments based on ASOs, or antisense oligonucleotides. These are short synthetic RNA molecules designed specifically for a certain gene. They do not change the DNA sequence itself, but influence the way the cell uses genetic information and produces proteins.
They can increase production of a missing protein, reduce production of a harmful protein or correct faulty splicing processes. One can think of them as linguistic editors of the genetic code.
The technology is already being used in other neurological diseases and is now at the forefront of epilepsy research as well. One of the most exciting aspects is the N-of-1 approach: developing a treatment intended for one child only, based on that child’s unique mutation. What was unimaginable only a few years ago is gradually becoming a real possibility.
") Dr. Michal TzadokPhoto: Sheba Medical Center
Dr. Michal TzadokPhoto: Sheba Medical CenterAlongside ASO treatments, gene therapy using viral vectors is developing rapidly. In this approach, genetically engineered viruses, usually AAVs, are used after losing their ability to cause disease. They serve as “messengers” that deliver genetic cargo to cells.
The vector enters the cell and delivers a correct copy of the missing gene, or a genetic sequence that regulates the activity of a faulty gene. Several such treatments are already in clinical trial stages, including for Dravet syndrome and other genetic syndromes that cause severe childhood epilepsy.
The challenges remain significant: how to reach an enormous number of nerve cells in the brain, how to ensure long-term effectiveness and how to prevent unexpected immune reactions. Still, the initial results are encouraging.
Making treatment more precise
It is also important to say what is less comfortable: not every genetic disease currently has a treatment. Innovative therapies are complex and very expensive to develop and produce, and many years may pass before they become available.
No less important, not all patients are referred for genetic evaluation in time. A delay in diagnosis can prevent access to targeted treatments, clinical trials or appropriate genetic counseling for the family.
In the past, doctors settled for trying to reduce seizures. Today, the goal is to understand the precise cause of the disease and treat it. In the not-too-distant future, the first question after an epilepsy diagnosis will not be, “Which medication should we give?” but rather, “What is the genetic mechanism causing the disease, and can it be corrected?”
For many families coping with severe, treatment-resistant epilepsy, this is no longer a distant promise. It is a revolution already underway.
Dr. Michal Tzadok is director of the Pediatric Epilepsy Center and the multidisciplinary TSC clinic at Sheba Medical Center, Tel Hashomer, and a senior lecturer at Tel Aviv University’s Gray Faculty of Medicine.